Annick Tumolo, licensed speech pathologist in San Francisco specializes in articulation and phonological disorders
Articulation is the way sounds are formed or produced using the articulators such as our tongue, teeth, and lips in a sequenced pattern. Phonology consists of our mental representation of the language rules that determine how sounds are combined to make words.
Children and adults with articulation and phonological disorders produce sounds differently from their age-matched peers or other adults. They may either have difficulty in the production of sounds and sound sequences of their language or have their own unique rule system that determines how they produce sounds and sequences.
A child person with an articulation disorder may have difficulty with the movements of the tongue, lips, teeth, jaw and vocal folds affecting their ability to be understood by others. A simple articulation disorder may consist solely of a lisp in which the person may not keep their top and bottom teeth together or have their tongue positioned correctly for accurate production of /s/ or /z/. Or an individual with cerebral palsy may have a severe articulation disorder in which they have difficulty coordinating the movements, controlling breathing and the voicing necessary to produce specific sounds/words.
A phonological disorder is when a person follows a sound system they have recreated in their mind that does not follow the typical sound system expected. All children learn to speak and start using what are called “phonological processes” in which they simplify their speech such as by saying “baba” for bottle, “wawa” for water etc. and as they learn more words it is considered normal for a child to delete final consonants for a short time (24-36 months of age) as they master the rules of production. It is when children begin using phonological processes that are not part of the normal rule system such as when they delete beginning consonants or use back sounds such as /g/ and /k/ to replace the sounds /t/ and /d/ that they may have a phonological disorder. For example, a child may say “gog” for “dog” or “goy” for “toy”. These are signs they may be demonstrating a phonological disorder. Additionally, a child may use a /t/ to represent the “sh” sound such as saying “tip” for “ship” but then they may say “ship” for “chip” thus demonstrating the correct articulatory production of “sh” in the latter example. Phonological disorders may differ from articulation disorders in that a child can produce sounds but uses the sounds in an atypical sequence without realizing they are doing so.
A child can have both an articulation and phonological disorder at the same time. A child with a history of chronic ear infections may have developed a unique sound system as a result of not being able to hear the accurate production of sounds as their speech was developing. Additionally, the child will have difficulty self-monitoring their speech productions and may not be articulating sounds correctly as well. At times, it is difficult to determine if a child has difficulty with articulation alone or if they have both an articulation and phonological disorder. The key to remember is that articulation has to do with forming sounds and phonology has to do with following a specific pattern of phonological rules.
Assessment
A speech language pathologist typically uses multiple testing procedures to determine whether an articulation and/or phonological disorder exist. Additionally, they can determine whether a child presents with a speech delay or disorder. Typically a delay is present when a child is following the developmental pattern of sound development but their use of normal phonological processes such as final consonant deletion continues to occur later than 36 months. On the other hand, a child who has a speech disorder does not produce speech normally. A child who is 8 and whispers using only vowel sounds has disordered speech.
During an evaluation it is crucial an SLP to determine an individual’s intelligibility through both observations and discussion with caregivers. Intelligibility refers to how well a person can be understood during spontaneous speech. It is necessary in determining the need and amount of speech therapy necessary. A person that is unintelligible will likely have more than 6 sounds in error. They may use more gestures and facial expressions to communicate. It is also important for the SLP to determine how the individual produces consonants, vowels and sequences of sounds in connected speech.
A child with a severe speech disorder may only use vowels to communicate. For example they may say “o ow I” for “go outside”.
It is the responsibility of the SLP to consider cultural differences during assessment. If the child is a non-native speaker of English they may be demonstrating a language difference and not a disorder. Typically, SLPs do not treat English speech sounds that are not found in a child’s native language such as the “th” sound.
Upon completion of a speech evaluation, the SLP determines the course of treatment that should be chosen ideally based on efficiency and effectiveness as determined by evidenced based practice. The ultimate goal of therapy is intelligibility, making sure the client becomes intelligible to everyone in his or her own natural environment.
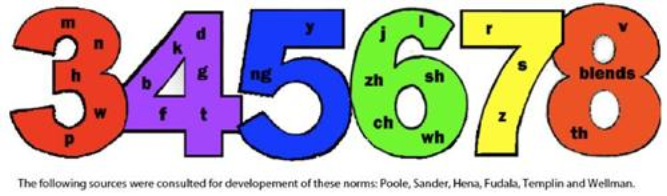
The following is the speech sound development for typically developing children ages 3-8